Randomized control trials (RCTs) represent the most reliable evaluation designs in social sciences, where laboratory experimental designs as in the natural sciences are not applicable. Akin to medical experiments, control trials ensure that control groups are really comparable and that we are comparing “like with like” when estimating impacts.
RCTs are based on two main components:
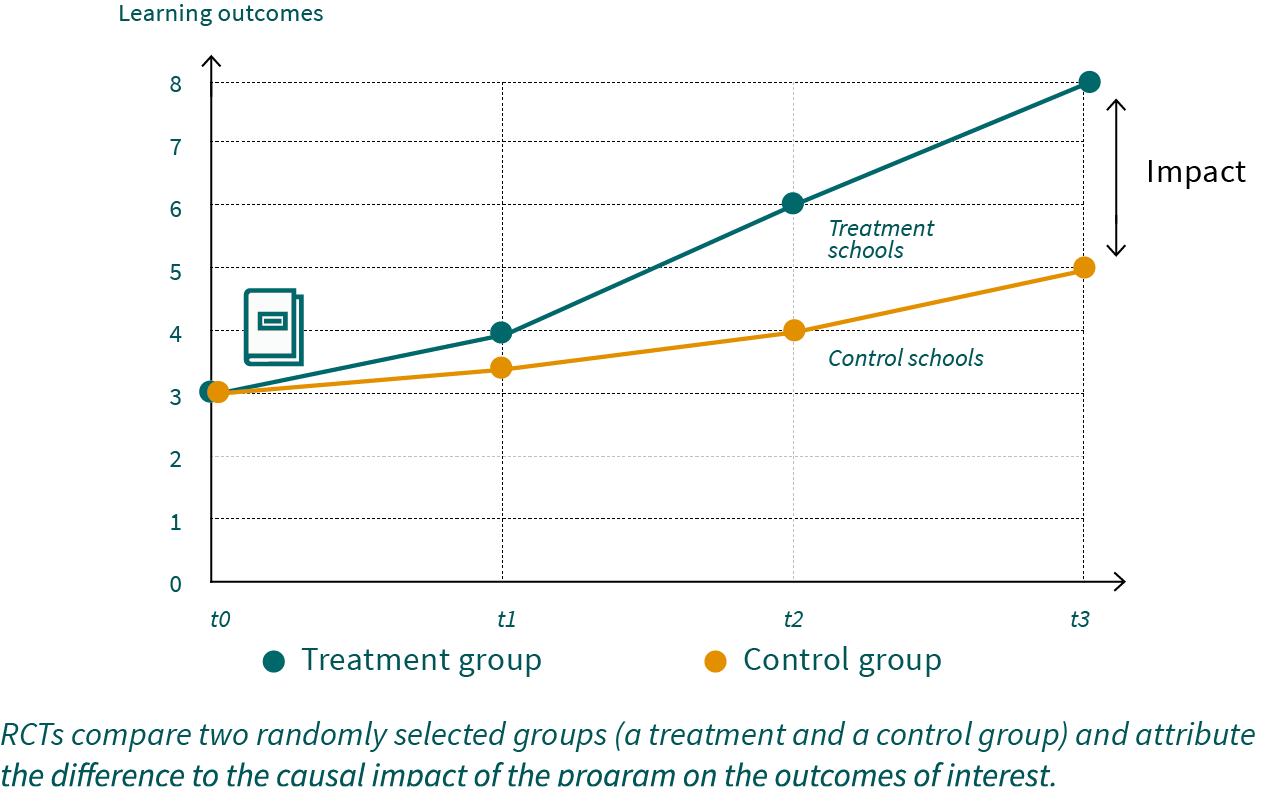
- Control group: There is a control group, used to construct the counterfactual outcome. The control group is not supposed to be covered by the program (the intervention, or treatment) nor should it by affected by spillovers (the fact that others are receiving the program).
- Randomized trial: Potential beneficiaries are randomly allocated either to the treatment group or control group. This ensures the equivalence, that is, the comparability of the groups on all observable and unobservable characteristics at baseline. If sample sizes are sufficiently large, randomization eliminates all confounding factors and selection bias, as both groups will differ only with regard to their treatment status. The outcomes of the program can therefore be compared on ceteris paribus conditions (other factors being equal).
RCTs therefore allow causal attribution, since observed differences in outcome variables can be attributed to the program itself. In other words, the observed difference between the program and the control groups represents the impact that has been generated because of the program. The randomization process furthermore ensures that impact estimates will be consistent without any assumptions. This is a major advantage as compared to observational quasi-experimental methods, which often rely on untestable ad-hoc assumptions. Therefore, control trials represent the most rigorous, unbiased method to measure impacts and establish causal effects and pathways.
Many development interventions are implemented at cluster level through schools, health posts, microfinance branches, village and community organizations, for instance. In such cases there may be compelling reasons to allocate all individuals or households that belong to the same cluster to the same kind of intervention status (treatment or control). For instance, all children of a given school should be allowed to participate in an educational intervention. Similarly, all households served by a given health post should benefit from an extended health program. In such situations, the random assignment of treatment versus control needs to be based on the level of the school or health posts (the cluster), instead of the individual or household. This prevents unfairness within clusters as well as the occurrence of spillovers. This method is referred to as cluster randomized control trials (C-RCTs). Whereas C-RCTs are conceptually like RCTs, they have relevant design implications, particularly with respect to sample size.